L-Carnitine
By Jens Allmer
(Updated: May 11, 2026)What L-carnitine is:
- L-carnitine is not a protein-building amino acid. It is derived from amino acids, but it has a different structure and function. It is also not a true vitamin, because the body can usually synthesize enough of it.
What L-carnitine does:
- Its main role is helping long-chain fatty acids enter mitochondria, where they can be broken down for energy. This transport system is called the carnitine shuttle.
Why “fat burning” claims are oversimplified:
- L-carnitine is necessary for fat metabolism, but that does not mean taking extra L-carnitine automatically makes a healthy person burn more fat. If the body already has enough, carnitine is usually not the limiting factor.
Who might actually need extra L-carnitine:
- Extra L-carnitine may be medically relevant in rare genetic carnitine transporter defects, some fatty-acid oxidation disorders, kidney disease or dialysis, premature infants, some severe illnesses, and with certain medications.
How to assess deficiency:
- Feeling tired is not enough to diagnose low carnitine. If deficiency is suspected, it should be assessed with blood tests such as free carnitine, total carnitine, and sometimes an acylcarnitine profile.
Supplement risks:
- L-carnitine supplements can cause nausea, stomach cramps, diarrhea, and a fishy body odor. High-dose or long-term use may also raise questions around TMAO production, seizure risk in susceptible people, kidney disease, and interactions with anticoagulants such as warfarin.
In short, L-carnitine is biologically important, but that does not automatically make extra L-carnitine useful. For most healthy adults, supplementation is probably unnecessary. This is also true for athletes. In specific medical situations, however, L-carnitine can become conditionally essential and should be evaluated properly.
What is L-Carnitine?
L-carnitine is not an amino acid! It’s also not a vitamin! Am I nitpicking? Misinformation is misinformation even if well intended.
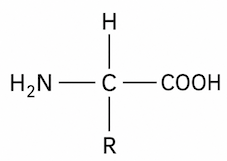
An amino acid is composed of a central carbon atom bonded to an amino group (-NH2), a carboxyl group (-COOH), a hydrogen atom, and a variable side chain (R-group). The R-group is different for all several hundred known amino acids. Around 20 of these amino acids are found in proteins so we call them proteinogenic amino acids.
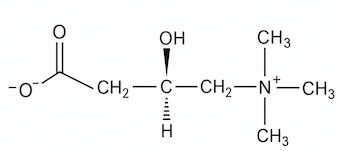
While l-carnitine loosely resembles the structure of an amino acid, it has a chain of carbon atoms separating the carboxyl group and the quaternary ammonium group. More importantly, the nitrogen atom in carnitine is connected to three methyl groups instead of hydrogen. This makes the nitrogen always positively charged, making it a quaternary ammonium compound.
L-carnitine not only loosely resembles an amino acid, but it is also synthesized in the body from two amino acids:
- L-lysine
- L-methionine
Thus, L-carnitine is an amino-acid-derived, conditionally essential metabolite involved in mitochondrial fatty-acid transport. Since it is usually sufficiently synthesized by the body, it is not an essential nutrient and, therefore, not a vitamin. However, in cases of a defect in the synthesis pathways, transport, or if there is an increased need, it can become an essential nutrient.
What does L-carnitine do in the body?
L-carnitine’s main job doesn’t involve building proteins. It acts like a transport molecule.
The body can use fat as fuel, but long-chain fatty acids cannot simply float into the mitochondrion, that performs the so-called β-oxidation (fat burning). They first need help crossing the inner mitochondrial membrane. This is where L-carnitine comes in. It temporarily binds fatty-acid groups, forming what biochemists call acylcarnitines, which can then be transported into the mitochondria. Once inside, the fatty-acid group is transferred to CoA and can then be broken down to produce ATP, the cell’s main energy currency.
This system is often called the carnitine shuttle. The basic logic is simple:
A long-chain fatty acid is attached to carnitine. The resulting molecuule (acylcarnitine) is moved into the mitochondrion. The fatty acid is released again and used for energy production.
The main enzymes involved are CPT1, CACT, and CPT2. CPT1 helps form acylcarnitines, CACT transports them across the inner mitochondrial membrane, and CPT2 converts them back into fatty acyl-CoA inside the mitochondrial matrix.
This is why L-carnitine is especially important in tissues that rely heavily on fatty acids for energy, such as skeletal muscle and heart muscle. These tissues do not use L-carnitine because it is magical, but because they often burn fat and therefore need an efficient way to move fatty acids into mitochondria.
L-carnitine also helps regulate the balance between free CoA and acyl-CoA molecules inside cells. That sounds technical, but the idea is straightforward: cells need free CoA for many metabolic reactions. By temporarily storing fatty-acid groups as acylcarnitines, carnitine helps prevent certain acyl groups from accumulating and interfering with metabolism. Some acylcarnitines can also be exported from mitochondria, which is one reason acylcarnitine profiles are useful in diagnosing disorders of fatty-acid oxidation.
So, in plain language:
L-carnitine helps move long-chain fatty acids into mitochondria so they can be burned for energy.
That does not mean that taking extra L-carnitine automatically makes a healthy person burn more fat. If the body already has enough carnitine, then carnitine is usually not the limiting factor. The bottleneck may instead be energy demand, exercise level, mitochondrial capacity, diet, hormones, or overall metabolic state. In other words, L-carnitine is important for fat metabolism, but it is not a simple “fat-burning switch.”
How to determine whether you need extra L-carnitine
Most healthy adults probably do not need extra L-carnitine. That may sound surprising if you have seen it sold as a fat-burning or energy-boosting supplement, but the body usually makes enough for normal needs. This is also why no official recommended daily intake has been established for carnitine. Healthy children and adults are generally able to synthesize enough from lysine and methionine. Compare that to vitamin D, which is actually a hormone and also produced in the body during exposure to UVB radiation. Even so, there is an official recommendation for vitamin D intake, since very few people manage to get enough from sun exposure these days.
Your first question should not be:
Could more L-carnitine give me more energy?
The better question is:
Is there a reason to think my carnitine status is too low?
Feeling tired, having low energy, or wanting to lose fat is not enough to diagnose a carnitine problem. These symptoms are common and can have a multitude of causes. Among them are lack of sleep, poor sleep quality, iron status, thyroid function, calorie intake, training load, infection, stress, diabetes, kidney disease, and many others. Taking L-carnitine without knowing whether carnitine is the limiting factor is like a shot in the dark.
There are, however, situations where carnitine deficiency is more plausible. These include primary carnitine deficiency, a rare genetic disorder affecting the carnitine transporter; secondary carnitine deficiency, for example due to kidney disease or hemodialysis; some inherited disorders of fatty-acid oxidation or organic-acid metabolism; premature birth; and some medications, including valproic acid and certain antabiotics wiht pivalate-containing as the active ingredient.
In more serious cases, low carnitine is not just being a bit tired. It can be associated with problems such as muscle weakness, episodes of low blood sugar, low ketone production during fasting, high ammonia, enlarged or weakened heart muscle, liver problems, rhabdomyolysis, or neurological symptoms during illness or fasting. These are medical warning signs, not supplement-shopping signs.
The direct way to assess carnitine status is a blood test. Clinically, this usually means measuring free carnitine, total carnitine, and sometimes the acylcarnitine profile. According to the NIH Office of Dietary Supplements, a plasma free carnitine concentration of 20 µmol/L or less, or a total carnitine concentration of 30 µmol/L or less, is considered abnormally low. The ratio of acylcarnitine esters to free carnitine can also be informative; a ratio of 0.4 or higher may suggest abnormal carnitine metabolism.
An acylcarnitine profile can be especially useful because it does not only ask “how much carnitine is there?” It also asks “what forms is it in?” This matters because abnormal acylcarnitine patterns can point toward problems in fatty-acid oxidation or organic-acid metabolism. In suspected primary carnitine deficiency, doctors may also check urine carnitine loss and may confirm the diagnosis with SLC22A5 genetic testing or a cellular carnitine-uptake test.
Diet alone is a weak guide. Red meat and other animal foods contain more carnitine than plant foods, so vegans and vegetarians usually consume much less carnitine. But this does not automatically mean they are deficient. The body can synthesize carnitine, and endogenous synthesis is usually sufficient in healthy people even when dietary intake is low.
So a practical approach would be
If you are healthy, have no relevant symptoms, no kidney disease, no known metabolic disorder, and are not taking medications known to lower carnitine, you probably do not need extra L-carnitine.
If there is a real suspicion of deficiency, test rather than guess.
In short
You do not determine L-carnitine need by asking whether you feel tired after work or whether a supplement label promises better fat burning. You determine it by context and, when needed, by measuring carnitine status. In healthy adults, extra L-carnitine is usually unnecessary. In specific medical situations, however, L-carnitine can become conditionally essential and should be evaluated properly.
If I choose to supplement, how should I do so and what are the risks?
If you still choose to supplement with L-carnitine, I would treat it as an experiment, not as a nutritional necessity. In a healthy adult, the goal should not be “as much as possible,” but the lowest reasonable dose for a clearly defined reason.
The first question is which form you are taking. L-carnitine or levocarnitine is the standard biologically active form. Acetyl-L-carnitine is a related form often marketed for brain, nerve, or fatigue-related purposes. Propionyl-L-carnitine is another related form sometimes discussed in cardiovascular or circulation contexts. Importantly, only the L-form is biologically useful. Products containing D,L-carnitine should be avoided because the D-form may interfere with L-carnitine transport and metabolism. For a more detailed overview of forms and absorption, see the Linus Pauling Institute page on L-carnitine.
For ordinary non-prescription use, supplemental doses commonly fall around 0.5–2 g per day. That does not mean everyone should take 2 g. A cautious approach would be to start around 500 mg per day, take it with or shortly after a meal, and only increase if there is a specific reason. Prescription dosing for confirmed deficiency is a different matter and should be managed medically. The NIH Office of Dietary Supplements provides a useful medical overview of carnitine, deficiency, and supplementation.
More is not automatically better. Oral carnitine supplements are absorbed rather poorly compared with carnitine from food. For supplement doses between 0.6 and 7 g, reported absorption is only about 5–25%. The rest may be excreted or metabolized by gut bacteria. So taking a very large dose does not simply mean that your muscles receive a very large amount of extra carnitine. See the Linus Pauling Institute section on supplemental L-carnitine absorption.
A practical routine would be:
Start low, take it with food, avoid mega-doses, and stop if there is no clear benefit.
Taking it with or just after meals may reduce stomach upset. If using more than one daily dose, spacing doses through the day is also reasonable. For medically prescribed levocarnitine, follow the instructions from your doctor or pharmacist. Mayo Clinic gives patient-facing information on levocarnitine use.
The common side effects are not dramatic, but they are real: nausea, vomiting, stomach cramps, diarrhea, and sometimes a fishy body odor. The fishy smell becomes more likely at higher intakes, especially around 3 g/day or more. The NIH consumer fact sheet on carnitine gives a simple overview of these side effects.
There are also people who should not casually experiment with L-carnitine. People with seizure disorders should be careful because high amounts may increase seizure risk. People with severe kidney dysfunction should also avoid unsupervised high-dose use, because carnitine and its metabolites may accumulate differently when kidney function is impaired. The NIH notes these cautions in its consumer fact sheet on carnitine, and Mayo Clinic also lists relevant medical cautions for levocarnitine.
There is also a cardiovascular question. Gut bacteria can convert unabsorbed carnitine into compounds such as trimethylamine, which the body can convert into TMAO. Higher TMAO has been associated with cardiovascular risk in some studies. This does not prove that every L-carnitine supplement causes heart disease, but it is a good reason not to take high-dose carnitine chronically without a convincing reason. The NIH health professional fact sheet discusses this issue in more detail.
Medication interactions matter too. If you take warfarin or a related anticoagulant, do not add L-carnitine casually. Official levocarnitine labeling reports increased INR in some warfarin users and recommends INR monitoring after starting levocarnitine or changing the dose. See the official DailyMed levocarnitine label.
Supplement quality is another issue. Dietary supplements are not approved for safety and effectiveness before they are sold in the same way medicines are. That does not mean all supplements are bad, but it does mean the label is not the same thing as proof. The FDA explains this in its page on using dietary supplements. If using a supplement, it is sensible to choose a product with independent quality testing, such as USP Verified or NSF certification.
So my conservative recommendation would be:
If you have a diagnosed deficiency or a medical reason, follow medical guidance. If you are a healthy adult experimenting with L-carnitine, stay in the low-dose range, avoid chronic high-dose use, avoid D,L-carnitine, take it with food, and stop if there is no clear benefit.
L-carnitine is biologically important. That does not automatically make extra L-carnitine useful. In metabolism, “important” and “limiting” are not the same thing.
Do athletes, bodybuilders, or runners benefit from extra L-carnitine?
Since L-carnitine helps transport long-chain fatty acids into mitochondria, it sounds logical that athletes might benefit from taking more of it. Bodybuilders may hope for better fat loss or recovery. Long-distance runners may hope for better fat use and endurance. But biology is not that simple.
For healthy athletes, the main question is not whether L-carnitine is important. It clearly is. The question is whether extra L-carnitine becomes the limiting factor. In most healthy people, the answer seems to be: probably not.
Studies in athletes and active adults have produced mixed results. Some studies reported improvements in markers such as VO2max, peak power, perceived exertion, lactate, muscle soreness, or recovery. Other studies found no meaningful improvement in endurance, fatigue, total work, heart rate, VO2max, or performance time. The NIH Office of Dietary Supplements summarizes the evidence as mixed and notes that no studies found improved moderate-intensity exercise performance.
This matters because most supplement marketing quietly jumps from:
L-carnitine is needed for fat metabolism
to:
More L-carnitine means more fat burning
That jump is not justified. If the body already has enough carnitine, adding more does not automatically make mitochondria burn more fat. Energy demand, training status, carbohydrate availability, mitochondrial capacity, hormones, and total calorie balance may be much more important.
There is one interesting exception: one study showed that long-term L-carnitine supplementation together with a large carbohydrate load increased muscle carnitine content and changed muscle fuel metabolism during exercise. But this was not a simple “take a capsule and burn fat” situation. It involved chronic supplementation with carbohydrate co-ingestion over many weeks. That is very different from casual supplement use.
For bodybuilders, the strongest argument is not muscle gain but possibly recovery. Some studies suggest that L-carnitine may reduce delayed-onset muscle soreness and markers of exercise-induced muscle damage. That could be relevant after hard training blocks. But this is not the same as proving that L-carnitine builds more muscle or directly increases strength.
For long-distance runners, the theoretical argument is better fat use and glycogen sparing. However, performance results are inconsistent. A runner who is already well nourished and not carnitine deficient should not expect L-carnitine to act like a legal endurance drug.
There are groups where benefit is more plausible, but these are not simply “healthy people who train hard.” They include people with diagnosed carnitine deficiency, some metabolic disorders, some dialysis patients, premature infants, and possibly patients with specific cardiovascular or metabolic conditions. In these cases, L-carnitine is closer to medical treatment than lifestyle supplementation.
There is also some evidence that L-carnitine may modestly reduce body weight in adults with overweight or obesity. A meta-analysis of 37 randomized controlled trials found small reductions in body weight, BMI, and fat mass, with the largest body-weight effect around 2 g/day. But the effect was modest, and this does not prove that L-carnitine is a powerful fat-loss supplement for lean, healthy athletes.
So, is there a clear “more is better” situation?
Not really.
A better summary is:
More L-carnitine may help when carnitine availability is genuinely low, when metabolism is clinically impaired, or possibly when recovery from muscle damage is the target. But in healthy athletes, bodybuilders, and runners, extra L-carnitine is not reliably shown to improve performance or fat loss. Important does not mean limiting, and biologically necessary does not mean supplementing more is better.
