Magnesium
By Jens Allmer
(Updated: May 11, 2026)- Why Magnesium Matters:
- Magnesium is needed for hundreds of vital reactions in our cells. It stabilizes ATP, the cell’s main energy currency, and helps regulate muscle contraction, nerve signaling, blood pressure, glucose metabolism, and heart rhythm. It also interacts closely with calcium, potassium, vitamin D, and parathyroid hormone (PTH).
- Magnesium Imbalances:
Low Magnesium (Hypomagnesemia): Can cause fatigue, weakness, tremor, muscle cramps, tingling, numbness, tetany, seizures, abnormal heart rhythms, and can make low potassium or low calcium difficult to treat.
High Magnesium (Hypermagnesemia): Is uncommon with normal kidney function but can occur with kidney disease or excessive intake from supplements, laxatives, or antacids. It can cause nausea, flushing, muscle weakness, reduced reflexes, low blood pressure, breathing problems, confusion, and in severe cases cardiac arrest.
- Magnesium balance is mainly regulated by intestinal absorption, storage in bone and soft tissues, and kidney excretion. When magnesium intake is low, the intestine absorbs a higher fraction and the kidneys conserve more magnesium. When magnesium intake is high, healthy kidneys excrete the excess.
- Bones and Magnesium Storage:
- Bones act as an important magnesium reservoir. Magnesium supports bone mineral structure, influences osteoblast and osteoclast (cells that build and break down bone tissue) activity, and is connected to vitamin D and PTH physiology. Poor magnesium status can therefore affect bone health indirectly as well as directly.
- Testing Magnesium Levels:
- A simple blood test can measure serum magnesium, but serum magnesium represents only a small fraction of total body magnesium. Understanding magnesium status may require additional tests such as urinary magnesium, kidney function, calcium, potassium, PTH, vitamin D, or bone-density testing depending on your specific situation.
- Sources of Magnesium:
- Magnesium is found in many foods, especially seeds, nuts, legumes, whole grains, leafy greens, and some mineral waters. Supplements differ strongly in elemental magnesium content, absorption, tolerability, and laxative effect. In people with kidney disease, magnesium supplementation should be approached carefully.
In short, Magnesium supports energy metabolism, muscle and nerve function, electrolyte balance, vitamin D physiology, and bone health. Maintaining a proper balance is important because both deficiency and excess can lead to serious health problems.
Magnesium
Magnesium is a vital mineral for muscles, nerves, heart, and bone structure. Most magnesium in the body is not floating freely in serum. A large fraction is stored in bone, much is inside cells, and only a very small fraction is present in the blood. Therefore, normal serum magnesium does not always reflect the whole-body magnesium stores. This makes magnesium status hard to assess with a simple blood test.
Elemental Magnesium
Magnesium has the atomic number 12, which means it contains 12 protons and 12 electrons. Its atomic weight is around 24.3, and the most abundant isotope has 12 neutrons. Magnesium has two outer electrons and, like calcium, belongs to the alkaline earth metals. It readily gives up these two electrons and commonly exists as Mg²⁺ in biological systems.
Because of this reactivity, elemental magnesium is not the nutritional form used by the body. In nature and in supplements, magnesium is found as part of compounds: magnesium oxide, magnesium carbonate, magnesium citrate, magnesium chloride, magnesium sulfate, magnesium glycinate, magnesium malate, magnesium lactate, and many others.
The compound matters because it changes the elemental magnesium percentage, solubility, tolerability, laxative effect, and sometimes the intended use. Magnesium oxide is chemically dense and cheap but poorly soluble and often inefficient for repletion. Magnesium citrate, chloride, lactate, glycinate, and malate are usually more practical everyday choices. Magnesium sulfate and hydroxide are often more relevant as laxatives, antacids, bath salts, or medical preparations than as elegant daily repletion forms. There might be a small uptake of Mg via the skin when bathing in magnesium sulfate, Epsom salts, or magnesium chloride. However, the uptake might be so small that it is difficult to measure. Hence, don’t rely on this method for repletion!
Why Magnesium Matters
Magnesium is involved in hundreds of biochemical reactions. One of its most important roles is that it stabilizes ATP, the cell’s main energy currency. In many reactions, the biologically useful form is not free ATP but Mg-ATP. This means magnesium is not merely a “mineral supplement” but a central participant in energy metabolism. Many enzymes also require magnesium as a cofactor to function properly. Enzymes catalyze biochemical reactions and many would be less efficient or inactive without magnesium. Not having sufficient Mg will therefore hamper hundreds of processes in the body. Clearly, you would be able to feel the effect if you are deficient in magnesium.
Magnesium also interacts closely with calcium and vitamin D physiology. Calcium is strongly associated with contraction, excitation, and signaling. Magnesium often counterbalances calcium by helping regulate calcium channels, membrane excitability, muscle relaxation, and nerve transmission. It is also needed for normal parathyroid hormone (PTH) function and for vitamin D metabolism. Severe magnesium deficiency can therefore lead to calcium and potassium disturbances that are difficult to correct unless magnesium is corrected as well.
Daily Requirement
Before looking at the daily requirement, we should remember that you can’t eat elemental magnesium. That would be dangerous because elemental magnesium is chemically reactive. Nutritional magnesium is provided as magnesium ions in foods or as magnesium compounds such as magnesium citrate, oxide, chloride, glycinate, lactate, malate, sulfate, and others. We just established that magnesium is highly reactive and that is why we will find it as a compound with other elements or molecules in nature. The bioavailability (how well your body can absorb the magnesium from one of the given compounds) varies greatly between the different compounds. Additionally, some compounds might cause issues while others may be targeted preferentially to certain tissues in the human body.
The recommended daily intake is usually given as milligrams of elemental magnesium, not as milligrams of the whole compound. This is important because 1 g of magnesium oxide contains far more elemental magnesium than 1 g of magnesium L-threonate, while the latter is often marketed for its alleged superior bioavailability to the brain (in my opininion, we need more data on that claim).
For adults, the commonly cited recommended intake is about 420 mg elemental magnesium per day for men and 320 mg elemental magnesium per day for women. Note that this refers to Mg from food. This is intake, not absorbed magnesium. Dietary magnesium absorption is often roughly in the range of 30–40%, although this varies depending on your current magnesium status, the food matrix, the chemical form, dose, intestinal function, and other dietary components. Using 35% as a rough estimate, 420 mg dietary magnesium corresponds to about 150 mg absorbed magnesium. This is why the supplement table below estimates how much of each compound would be required to absorb about 150 mg magnesium.
The tolerable upper intake level for supplemental magnesium is usually given as 350 mg/day for adults. This upper limit applies to magnesium from supplements and magnesium-containing medications, not to magnesium naturally present in foods. Food magnesium rarely causes toxicity in people with normal kidney function because the kidneys can excrete excess magnesium. Supplements and laxative/antacid forms are different because they can deliver concentrated magnesium loads.
The daily recommended value of magnesium is 420 mg elemental Mg for a male and 320 mg for a female. Now, this should be scaled by size, but there is no information on that. The RDA is given as what you need to take in not what is actually absorbed. The estimate for the RDA is 35% absorption. This means a male of average size would need to absorb 150 mg Mg per day. Since Mg comes in different forms with varying bioavailability, cost, and side effects, it is important to make an informed choice. Some Mg forms might be for special cases such as Magnesium L-threonate, which is marketed for its ability to cross the blood-brain barrier and improve cognitive function. Other forms, like magnesium sulfate, are mostly used as laxatives or bath salts. There is nothing wrong with mixing different forms to cover different needs. However, supplementing with Mg should keep the dietary input of magnesium in mind so we don’t take in too much. Excessive amounts of Mg can be dangerous. The tolerable upper intake level (UL) for supplemental magnesium is 350 mg per day for adults (keep in mind that your weight matters here and adjust accordingly). This UL applies more to magnesium from supplements and not as much to magnesium naturally present in food. However, like any other compound, the levels in the body need to be tightly controlled.
Use the following table to get a feel of how much of the various Mg compounds correspond to 150 mg of elemental Mg in terms of bioavailability. Cost may be an issue as well, but prices vary. Some Mg compounds taste awful so you might want to avoid them or mix them with something tasty.
| Compound | Elemental Mg % | Assumed absorption | g compound to contain 420 mg elemental Mg | g compound to absorb ~150 mg Mg | Practical interpretation |
|---|---|---|---|---|---|
| Magnesium oxide | 60.3% | ~4–10% | 0.70 g | 2.5–6.2 g | Chemically dense, biologically inefficient |
| Magnesium hydroxide | 41.7% | ~10–15% | 1.01 g | 2.4–3.6 g | More laxative/antacid than elegant repletion |
| Magnesium carbonate | 28.8% | ~10–20% | 1.46 g | 2.6–5.2 g | Acid-dependent; can act antacid/laxative |
| Magnesium chloride, anhydrous | 25.5% | ~30–40% | 1.65 g | 1.5–2.0 g | Efficient if truly anhydrous; soluble |
| Magnesium citrate | ~16.0% | ~25–35% | 2.6 g | 2.7–3.8 g | Good common compromise; can loosen stool |
| Magnesium malate | ~15.5% | ~30–40% | 2.7 g | 2.4–3.2 g | Reasonable general supplement |
| Magnesium bisglycinate / glycinate | ~12.0% | ~30–40% | 3.5 g | 3.1–4.2 g | Often well tolerated; check for “buffered” oxide mixtures |
| Magnesium chloride hexahydrate | 12.0% | ~30–40% | 3.5 g | 3.1–4.2 g | Soluble but bulky |
| Magnesium lactate dihydrate | 10.2% | ~30–40% | 4.1 g | 3.7–4.9 g | Good absorption category but bulky |
| Magnesium sulfate heptahydrate / Epsom salt | 9.9% | ~10–20% | 4.2 g | 7.6–15.2 g | Mostly laxative/bath salt context |
| Magnesium taurate | ~8.9% | ~25–35% | 4.7 g | 4.8–6.7 g | Low Mg density; heart claims not proven as targeting |
| Magnesium aspartate | ~8.4% | ~30–40% | 5.0 g | 4.5–6.0 g | Good absorption category but low Mg density |
| Magnesium L-threonate | ~8.3% | ~25–35% | 5.1 g | 5.2–7.2 g | Very low Mg density; CNS-marketed, inefficient for Mg repletion |
| Magnesium gluconate | ~5.4% | ~25–35% | 7.8 g | 7.9–11.1 g | Gentle but extremely bulky |
Magnesium Uptake
Magnesium is found in many foods, so getting Mg should not usually be a problem unless the diet is highly refined or restricted. However, the amount absorbed depends on the food source, magnesium status, gut health, dose, and chemical form.
Food magnesium is often absorbed at about 30–40%, but this is not a fixed number. If body magnesium is low, fractional absorption may increase. There are active and passive mechanisms for magnesium absorption. TRPM6/7 is the primary active transporter in the gut and channels Mg through the gut cells into the blood stream in case of low magnesium status. If intake is high, the percentage absorbed may decrease. This is one reason why simply taking huge doses is not a good strategy. More is not always better, and too much supplemental magnesium often causes diarrhea before it leads to repletion.
A simplified view of magnesium uptake
While there is more to Mg uptake than displayed in the diagram below, it illustrates key concepts. We are not discussing the active uptake through TRPM6 and TRPM7 channels in the gut, which happens in case of low Mg status. The interaction with other minerals such as Ca and Na, and the effect of phytates, oxalates, fiber, and vitamin D are not discussed here either.
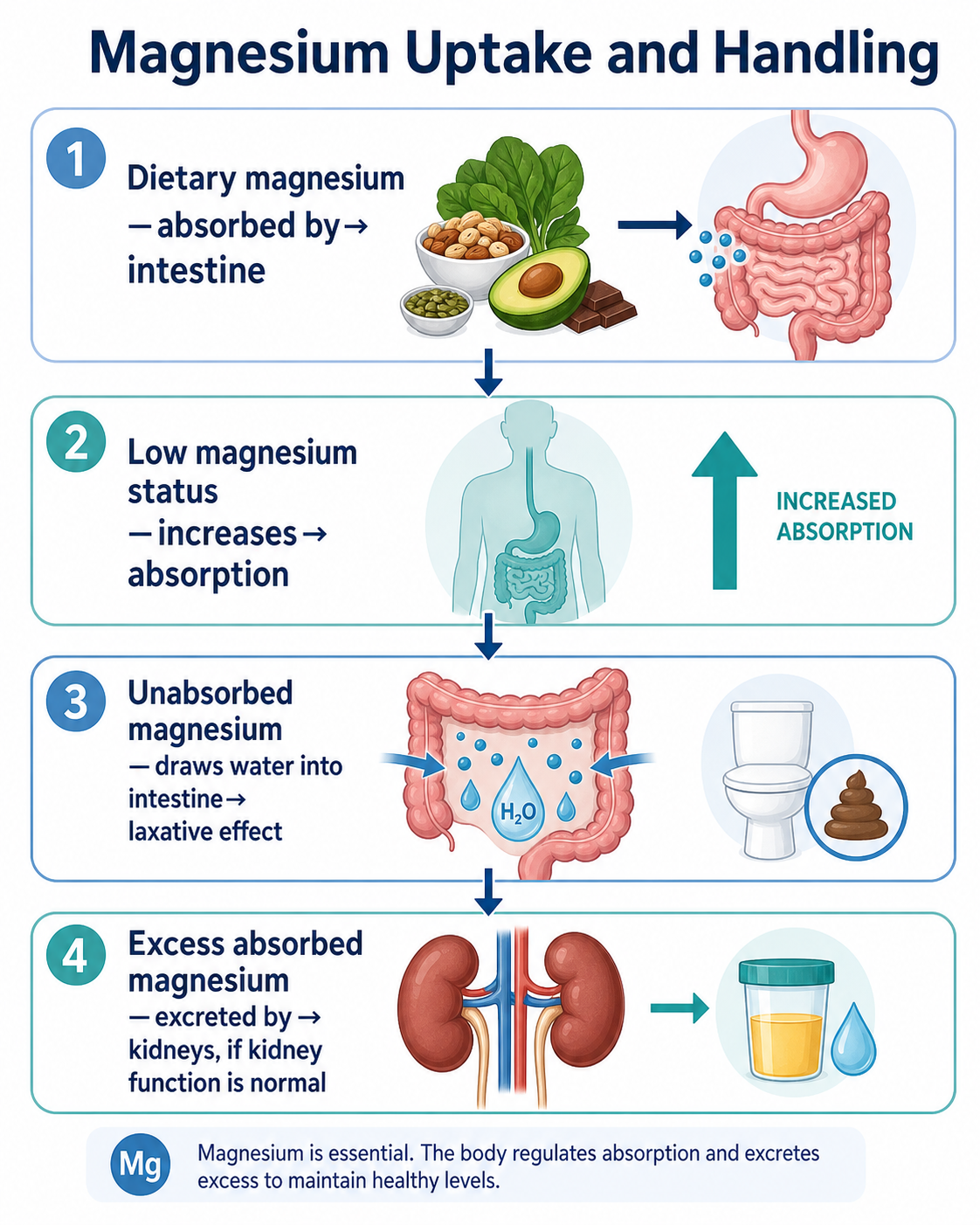
This simple view, however, explains why various forms of magnesium, such as citrate, hydroxide, oxide, and sulfate can loosen stool or act as laxatives.
Magnesium Supplements
As discussed above, magnesium compounds differ in elemental magnesium percentage, absorption, tolerability, taste, cost, and side effects. Some compounds are chemically dense but biologically inefficient. Others are bulky but better tolerated. Some are mainly used as laxatives or antacids. Others are marketed for special purposes such as sleep, muscle relaxation, or cognition.
In case the table above is too detailed, here is a simplified summary of common magnesium compounds:
| Goal | Best choices |
|---|---|
| Cheap, high elemental Mg but poor absorption | Oxide |
| General supplement, good balance | Citrate, glycinate/bisglycinate, chloride, lactate |
| Gentle on stomach | Glycinate/bisglycinate, lactate, gluconate |
| Constipation | Citrate, hydroxide, sulfate |
| Avoid laxative effect | Glycinate/bisglycinate, malate, lactate |
| Brain/CNS-oriented marketing | L-threonate |
| Maximum elemental Mg per gram | Oxide, hydroxide, carbonate |
| Most “efficient” absorbed everyday forms | Citrate, chloride, lactate, glycinate/aspartate |
Calcium, Magnesium, and “Too Much Supplementation”
With calcium, the central concern is often hypercalcemia, kidney stones, vascular calcification questions, or abnormal bone resorption. With magnesium, the practical problem is often different: too much supplemental magnesium first causes gastrointestinal symptoms, especially loose stool or diarrhea. Serious toxicity is uncommon unless kidney function is impaired or very high magnesium doses are taken.
However, magnesium should still be treated carefully. High-dose magnesium can interact with medications and can impair the absorption of certain drugs if taken at the same time. This is especially relevant for some antibiotics, bisphosphonates, thyroid medication, and other compounds that bind divalent cations (2+). In practical terms, magnesium supplements are often separated from such medications by several hours, depending on the medication instructions.
People with kidney disease should be especially careful with magnesium supplements because the kidney is the main route for removing excess magnesium.
Magnesium-Rich Foods
Most real foods contain at least some magnesium, but the richest common sources are seeds, nuts, legumes, whole grains, and leafy green vegetables. Chlorophyll contains magnesium, which is one reason green plant foods are often good sources. Whole grains contain more magnesium than refined grains because much of the magnesium is lost when bran and germ are removed. Meats and dairy are not particularly rich in magnesium.
| Food | ~Approx. ~Mg per 100 g / 100 mL | Practical interpretation |
|---|---|---|
| Pumpkin seeds | ~550–590 mg/100 g | Very high; one of the densest common food sources |
| Chia seeds | ~330–390 mg/100 g | Very high; also high in fiber |
| Cashews | ~260–290 mg/100 g | High |
| Almonds | ~270–280 mg/100 g | High |
| Peanuts | ~160–180 mg/100 g | Moderate to high |
| Peanut butter | ~150–170 mg/100 g | Moderate to high; depends on product |
| Spinach, boiled | ~85–90 mg/100 g | High for a vegetable; cooking concentrates the leaves |
| Black beans, cooked | ~65–75 mg/100 g | High for a cooked staple food |
| Edamame, cooked/shelled | ~60–65 mg/100 g | Moderate to high |
| Whole grains, cooked brown rice | ~40–45 mg/100 g | Moderate |
| Whole grains, oatmeal/porridge | ~35–45 mg/100 g | Moderate; dry oats are much denser before cooking |
| Soy milk | ~20–30 mg/100 mL | Variable but useful |
| Mineral water | ~1 to >120 mg/L | Highly variable; check bottle label |
| Chicken breast, roasted | ~25–31 mg/100 g | Relevant contribution but not Mg-rich |
| Beef, lean/ground cooked | ~20–25 mg/100 g | Relevant contribution but modest |
| Pork chop/loin, cooked | ~25–30 mg/100 g | Relevant contribution but modest |
| Turkey breast, roasted | ~25–30 mg/100 g | Relevant contribution but modest |
| Salmon, cooked | ~30–31 mg/100 g | Modest; slightly better than many meats |
| Halibut, cooked | ~28 mg/100 g | Modest |
| Egg, whole | ~10–12 mg/100 g | Low |
For most people, the best magnesium strategy is not to chase a single miracle compound but to combine magnesium-rich foods with a well-tolerated supplement only if needed. A diet with legumes, nuts, seeds, whole grains, and leafy greens often already provides substantial magnesium.
Magnesium Imbalances
Magnesium balance is important because too little and too much magnesium can both cause health problems.
Hypomagnesemia (low magnesium)
Hypomagnesemia means that magnesium in the blood is too low. It can occur because of poor intake, chronic diarrhea, malabsorption, alcohol use disorder, uncontrolled diabetes, certain kidney problems, diuretics, proton-pump inhibitors (remember the active transport pumps for Mg in the gut?), nephrotoxic drugs, chemotherapy drugs such as cisplatin, and other conditions.
Symptoms can include loss of appetite, nausea, vomiting, fatigue, weakness, tremor, muscle cramps, muscle fasciculations, numbness, tingling, tetany, and seizures in severe cases. Neurological and psychological symptoms such as irritability, personality changes, lethargy, or confusion can also occur.
Cardiac effects are especially important. Magnesium is involved in electrical stability of the heart. Low magnesium can contribute to arrhythmias and is classically associated with problems such as ventricular irritability and torsades de pointes. Low magnesium is also clinically important because it can make low potassium and low calcium difficult to correct.
Hypermagnesemia: High Magnesium
Hypermagnesemia means that magnesium in the blood is too high. It is uncommon in people with normal kidney function, because healthy kidneys usually excrete excess magnesium. Supplementing with too much Mg usually first leads to gut problems such as diarrhea, which then limits further absorption. The risk is much higher in kidney failure or when people take large amounts of magnesium-containing laxatives, antacids, or supplements despite obvious diarrhea and kidney problems.
Symptoms of high magnesium can include nausea, flushing, muscle weakness, reduced reflexes, low blood pressure, sleepiness, confusion, impaired breathing, and, in severe cases, cardiac arrest. Severe hypermagnesemia is a medical emergency.
This is why magnesium supplementation should not be treated as automatically harmless. Food magnesium is usually safe in healthy people, but high-dose supplemental magnesium is different, especially in people with reduced kidney function.
The Bone as Magnesium Storage
Similar to calcium, magnesium is stored partly in bone. Roughly half of the body’s magnesium is found in bone, about a quarter in muscle, and the rest in soft tissues, blood cells, and serum. This means that magnesium status cannot be understood by looking only at serum magnesium. Imagine that serum magnesium diminishes. Since it is important, it will be replenished from the skeleton. This means that bone will be sacrificed to keep serum levels normal. Bone demineralization then occurs, which may eventually lead to osteoporosis. Therefore, it is important to not only assess the magnesium status in serum.
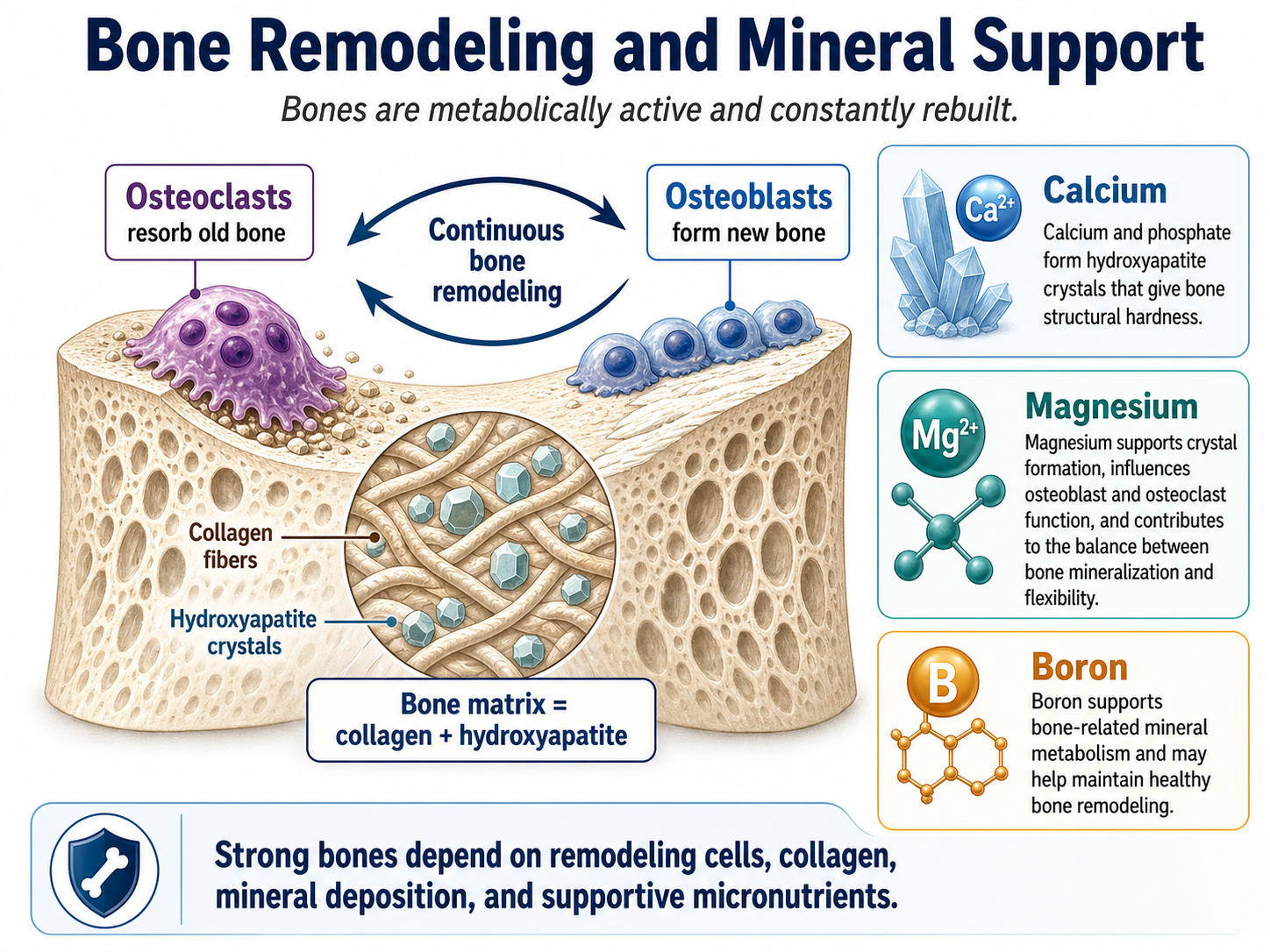
Bones are not built once and then forgotten. They are metabolically active and constantly remodeled. Osteoblasts build new bone tissue, while osteoclasts break down bone tissue. Calcium in the form of hydroxyapatite crystals provides structural hardness together with collagen. Magnesium is also part of this mineral system. It influences bone crystal formation, bone cell function, and the relationship between bone mineralization and bone flexibility.
Magnesium deficiency can negatively affect bone health through several mechanisms. It may impair PTH secretion or PTH action, interfere with vitamin D metabolism, increase inflammation, alter osteoblast and osteoclast behavior, and contribute to poor mineralization. This connects magnesium status with calcium status, vitamin D status, and bone strength.
A simple view of bones in relation to magnesium
Magnesium is not just “another electrolyte.” It is part of the mineral network that includes calcium, phosphate, PTH, calcitriol, kidney function, and bone remodeling. While bones store calcium, they also store magnesium and may need some boron for additional hardness. PTH and calcitriol increase calcium in the blood and vitamin K2 ensures it is deposited in the bones where it belongs. Low magnesium can impair PTH and calcitriol thereby leading to hypocalcemia and potentially to osteoporosis.
Magnesium Regulation
Calcium regulation is strongly driven by PTH, calcitriol, calcitonin, bone exchange, intestinal absorption, and renal handling. Magnesium regulation overlaps with this but is not identical. Magnesium balance is mainly maintained by three systems:
- Intestinal absorption
- Bone and intracellular storage
- Kidney excretion or conservation
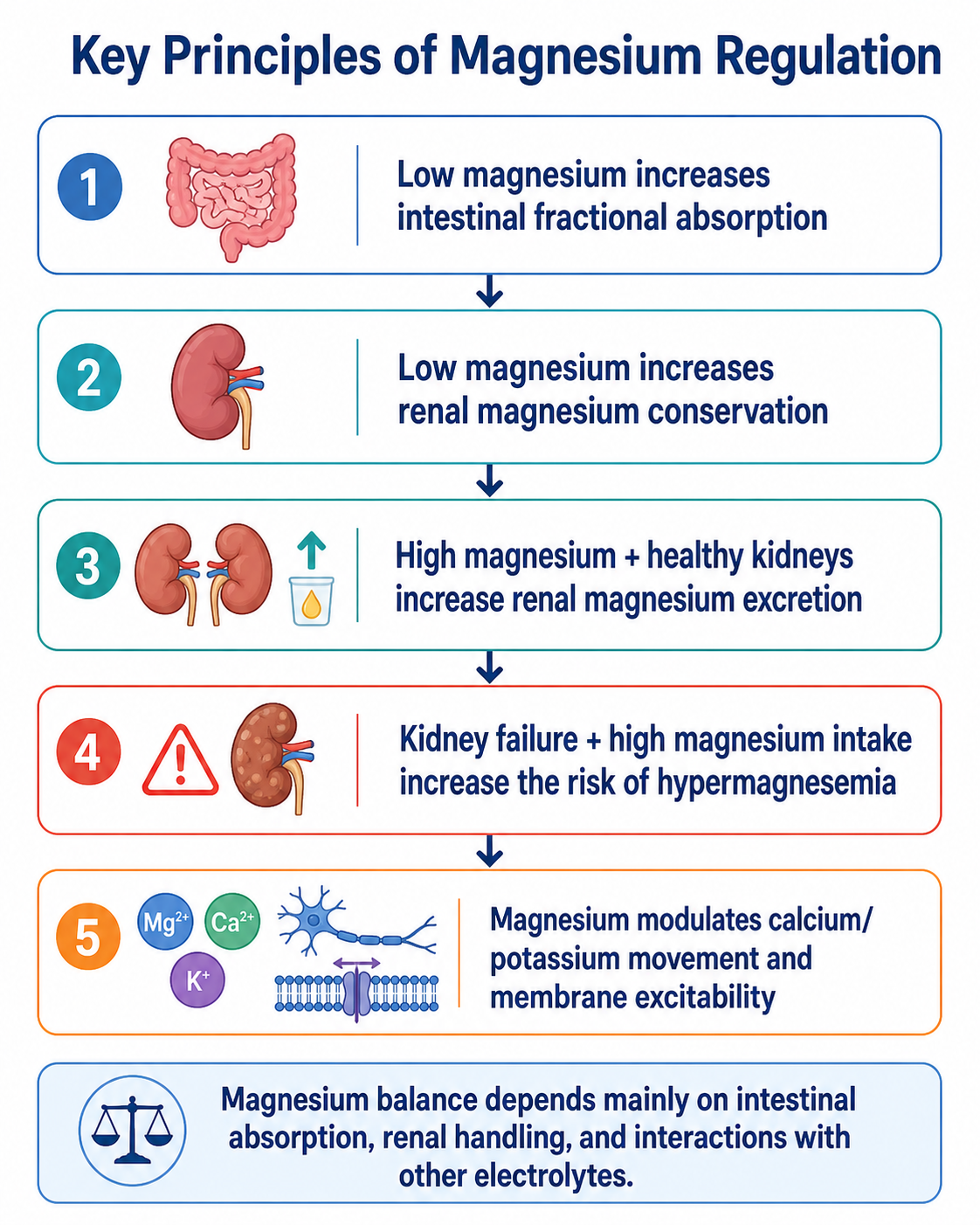
The kidney is especially important. If magnesium intake is low, the kidney can conserve magnesium. If magnesium intake is high and kidney function is normal, the kidney can excrete more magnesium. This is why hypermagnesemia is rare with normal renal function but dangerous in kidney failure.
The intestine also adapts. When magnesium status is low, fractional absorption can increase. When intake is high, the absorbed fraction may decrease. Absorption occurs through both passive paracellular transport and active transcellular mechanisms, especially involving magnesium channels such as TRPM6 and TRPM7.
Splified regulatory view is
The important difference from calcium is that there is no simple “magnesium version” of calcitonin that can be used to explain the whole system. Magnesium is more diffusely regulated by absorption, storage, and excretion.
Magnesium and Vitamin D
In the calcium article, calcitriol is central because it strongly increases calcium absorption from the intestine. Magnesium is linked to this system in a different way: magnesium is needed for normal vitamin D metabolism and function.
Vitamin D from the skin or diet must be converted first to calcifediol and then to calcitriol. Magnesium is involved as a cofactor in enzymes that participate in vitamin D metabolism. If magnesium is severely deficient, vitamin D activation and PTH physiology may not work optimally. This can indirectly disturb calcium balance and bone health.
Thus, calcium, vitamin D, and magnesium should not be thought of as isolated nutrients. They form a connected network. This also means that supplementing vitamin D while ignoring severe magnesium deficiency may be biologically incomplete in some situations.
Magnesium Levels in the Blood and Testing Magnesium Status
Magnesium status is harder to judge than calcium status because only a very small part of the body’s magnesium is found in the blood. Most magnesium is inside cells such as muscle cells, or stored in bone. This means that a normal blood magnesium value can be reassuring, but it does not always prove that total body magnesium stores are optimal.
In blood, magnesium exists in several forms. The most biologically active form is ionized magnesium, but routine laboratory testing usually measures total serum magnesium.
| Magnesium form in blood | What it means |
|---|---|
| Ionized magnesium | The free, biologically active fraction |
| Protein-bound magnesium | Mostly bound to albumin |
| Complexed magnesium | Bound to small molecules such as phosphate, citrate, or bicarbonate |
| Total serum magnesium | The sum of these forms; this is what is usually measured clinically |
Typical total serum magnesium is often around 1.7–2.4 mg/dL, although the exact reference range depends on the laboratory. Hypomagnesemia is commonly considered at <1.8 mg/dL, while hypermagnesemia is often considered at >2.6 mg/dL. However, the number should not be interpreted in isolation. Symptoms, kidney function, medication use, calcium, potassium, and the clinical situation matter.
The important limitation is this: serum magnesium is a small window into a much larger magnesium system. If serum magnesium is clearly low, this is meaningful. If it is clearly high, this is also meaningful, especially in kidney disease. But a normal serum magnesium value does not completely exclude magnesium depletion, because the body may maintain blood magnesium for some time by drawing on intracellular and bone stores.
Therefore, magnesium testing should be interpreted as part of a broader picture rather than as a single yes/no answer.
| Test or marker | What it can tell you |
|---|---|
| Serum magnesium | Common first test; detects clear low or high blood magnesium |
| Ionized magnesium | More directly reflects biologically active magnesium, but is less commonly available |
| RBC magnesium | Sometimes used as a rough intracellular marker, but interpretation is not standardized everywhere |
| Urinary magnesium | Helps distinguish low intake/poor absorption from kidney magnesium wasting |
| Fractional excretion of magnesium | Useful when renal magnesium wasting is suspected |
| Kidney function tests | Essential because impaired kidneys increase the risk of magnesium accumulation |
| Calcium and potassium | Important because low magnesium can make low calcium or low potassium difficult to correct |
| PTH and vitamin D tests | Useful when magnesium, calcium, vitamin D, and bone regulation appear connected |
| ECG | Relevant when arrhythmia or severe electrolyte disturbance is suspected |
| DXA/BMD testing | Useful for bone health, but not specific for magnesium |
In practice, a simple serum magnesium test is a reasonable starting point. But when symptoms, medication history, kidney function, or calcium/potassium abnormalities suggest a deeper problem, additional tests may be needed. Magnesium status is best understood together with diet, gastrointestinal function, kidney function, medications, calcium, potassium, vitamin D, PTH, and bone health.
